Editorial perspective from Kallisio. This article is a contribution to the conversation about workflow design in radiation oncology. It is not clinical guidance, and it is not a recommendation about any specific device or product for any individual patient.
A question worth taking seriously
In early January, Ben Freeberg published an essay on the Oncology Ventures Substack titled “What if Cancer Care Operated Like The Ritz-Carlton + WiFi Comedy”. The piece argued that healthcare, and cancer care in particular, has more to learn from how other service industries design for the people they serve than the field tends to admit. Toward the end of the essay, Freeberg asked his readers a direct question: what is the most broken part of the oncology workflow that nobody is fixing yet?
It is a fair question, and I want to take it seriously. I have spent more than thirty years in medical technology, much of it inside radiation oncology, and the question Freeberg is asking is the one I think about most days.
Freeberg’s framing draws on three companies known for service design: Ritz-Carlton, Apple, and Amazon. He asks what cancer care might look like if it borrowed their respective strengths, namely empowered front-line workers, radical simplicity, and end-to-end visibility. The proposition is not that cancer care can be turned into hospitality. The proposition is that principles of service design are translatable, and that many of the friction points patients experience are not inherent to the disease. They are inherent to how the workflow has been built around the disease.
That distinction matters. Once you accept it, the question becomes very specific: where exactly does the workflow break down, and why has nobody fixed it?
The gap between precision planning and precision delivery
Modern radiation oncology has become extraordinarily good at planning care. Over the past two decades the field has delivered sub-millimeter target volume definition, highly conformal dose sculpting through IMRT, VMAT, and proton therapy, sophisticated imaging and image-guided positioning, and increasingly capable adaptive replanning and AI-assisted contouring. These are real achievements, built by clinicians, physicists, and engineers over many years of careful work.
And yet there is a gap that persists, and it rarely gets named clearly: the gap between the precision designed into the plan and the precision with which that plan is executed across thirty or more daily fractions.
A head and neck radiotherapy course typically spans six to seven weeks of daily treatment. Across all of those sessions, the precision of the plan depends on a chain of conditions being reproduced day after day, including the patient’s position, the geometry of healthy structures relative to the target, the equipment, the team, and the timing. Each link in that chain has its own variability. Each has been refined over time. But the cumulative variability across the chain is real, and it is what clinical teams quietly manage every day.
This is not a failure of clinicians. The opposite is true. Clinical teams routinely deliver excellent care despite the variability the system hands them. The question I keep coming back to is whether more of that variability could be designed out upstream, so that downstream execution becomes easier rather than harder.
Why this gap has been allowed to persist
Freeberg’s essay names something that applies directly here: the friction points patients experience are often structural, not clinical. The same is true of the gap I am describing. It persists not because clinicians have ignored it, but because it sits in an organizational blind spot.
- It is not a new therapy, so pharmaceutical companies do not own it.
- It is not a linear accelerator or a planning system, so equipment vendors do not prioritize it.
- It is not an IT system, so enterprise teams do not engage with it.
- It is not, on its own, a high-margin line item, so administrative attention drifts elsewhere.
So clinicians adapt. They build local workarounds. They develop institutional knowledge. They compensate for variability the system never resolved. And the patient experience absorbs whatever the workflow could not.
This is the structural reason that innovation in the supportive layer of cancer treatment, the layer that determines how patients experience precision day to day, has lagged behind innovation in the therapy itself. It belongs to no single discipline, so no single discipline drives it forward.
What Ritz-Carlton, Apple, and Amazon actually teach
Freeberg’s analogies are not, in the end, about hotels or shopping. They are about three principles of service design that translate well to cancer care.
Ritz-Carlton: empower upstream design so downstream friction disappears. The famous policy that any employee can spend up to two thousand dollars to solve a guest’s problem is not really about money. It is about removing the layers of approval that would otherwise prevent a problem from being solved now it appears. The applied principle is to solve problems as close to their origin as possible.
Apple: remove intimidation through human-centered design. Apple’s product philosophy is not minimalism for its own sake. It is the recognition that complexity is the enemy of trust. The applied principle is that when a system feels intimidating, people disengage from it. When it feels simple, they engage with it more deeply.
Amazon: make the process predictable and visible. The tracking systems are not really about packages. They are about removing the cognitive load of uncertainty. The applied principle is that people tolerate complexity far better when they have visibility into what is happening and what comes next.
Translated into cancer care, these three principles point in the same direction: engineer the variability out of the system upstream, so that the patient experience downstream becomes predictable, simple, and trustworthy. Or, as Freeberg himself put it, the goal is to translate, not to copy.
What this means inside radiation oncology
The most generative reframing of Freeberg’s question, for our field specifically, is this: what if the assumption that patients must adapt to the treatment system is itself the problem?
In radiation oncology, that assumption shows up in small ways and in large ones. Patients often arrive at simulation with limited prior context about what is going to happen. Many supportive elements of treatment are organized around what is feasible to deliver rather than around what would be optimal to receive. Variability is managed by clinical teams rather than designed out of the workflow.
None of this is unique to oncology. It is the natural shape of any complex system that has grown around a powerful core technology, in this case the linear accelerator and the planning workflows that feed it. The core technology is brilliant. The wrapper around it has not always been redesigned to match.
The opportunity, then, is not to revolutionize radiation oncology. It is to bring service-design discipline to the layers that surround the radiation itself, namely the human-device interface, the daily setup, the patient’s lived experience over six or seven weeks of treatment, and the points of friction the clinical team currently absorbs by sheer force of competence.
That is where we have chosen to focus at Kallisio.
What we are trying to do
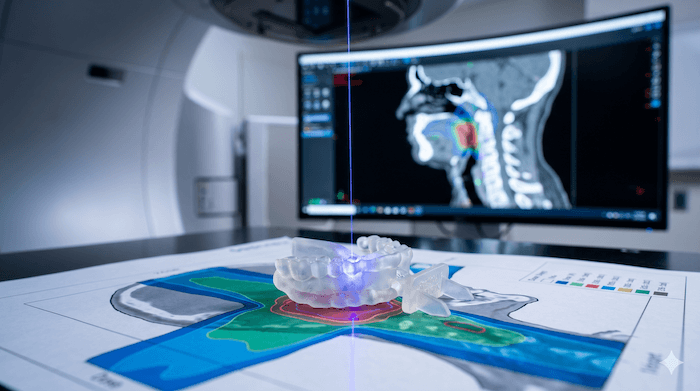
Our purpose is straightforward, and it informs how we approach the workflow question. We are trying to reduce the unnecessary burden patients experience as a byproduct of treatment, rather than because of the disease itself. Our first product, Stentra™, is an FDA 510(k)-cleared and CE-marked patient-specific intraoral immobilization and positioning device for head and neck radiation therapy, billable under CPT 77334. It is designed to fit inside existing radiation oncology workflows, present in CT simulation, captured in the planning dataset, used across all fractions, and requiring no changes to treatment planning systems. We have collaborated with Stanford Health Care on clinical implementation, and we work with other cancer centers across the United States. In May, Stentra was named Best New Radiology Technology Solution in the 2026 MedTech Breakthrough Awards.
We deliberately designed Stentra as a standard accessory rather than as a disruptive product. That choice was strategic, not technical. The radiation oncology workflow does not have room for products that require IT integration, physics re-architecture, or institutional change-management cycles. The fastest way to deliver upstream design to a system that needs it is to do so without asking the system to reorganize itself.
Whether Stentra is the right approach for any individual case is a clinical decision that belongs to the treating team. What I do believe, and what I think the workflow question really invites everyone in this field to consider, is that more of supportive care could be designed rather than absorbed.
A closing thought
Freeberg’s essay closes with a line that has stayed with me: let us acknowledge where our friction points are and how we can redesign around them.
That is the right framing. The most broken parts of cancer care are not the therapeutic decisions. The therapeutic decisions, overall, are getting better year after year. The broken parts are the structural assumptions that have crystallized over decades, about who owns supportive care, about what variability is acceptable, about what patients should adapt to.
Those assumptions are addressable. Not all at once, not by any single company, and not without close collaboration with the clinical teams who do this work every day. But they are addressable. And the longer the question of who fixes the gap between precision planning and precision delivery sits in the organizational blind spot, the longer patients absorb what the workflow did not.
That, to me, feels like a worthwhile thing to work on.
— Rajan Patel
Founder and CEO, Kallisio
Kallisio is a medtech company developing patient-specific, technology-enabled solutions to support precision radiation oncology. Learn more at kallisio.com.


