As 2025 comes to a close, the medical manufacturing landscape looks markedly different than it did just five years ago. Personalized medicine, once synonymous with high customization and long delays has matured into a practical clinical capability. Market analyses now estimate the healthcare additive manufacturing sector to be growing at approximately 18–20% annually, driven by hospitals adopting digital workflows and leveraging distributed manufacturing partners rather than relying solely on traditional labs.¹
What ultimately defined progress in 2025 was not printer resolution, material selection, or even unit cost, it was turnaround time. For years, the industry focused on whether patient-matched devices could be produced. The more clinically relevant question has now become when they arrive.
In oncology, customization that delays treatment initiation is rarely acceptable. The next frontier of personalized medicine is therefore not improved geometry alone, it is speed aligned with clinical timelines.
How Does 3D Printing Reduce Time to Treatment?
Direct answer: By replacing physical impressions and manual fabrication with a fully digital scan-to-print workflow, clinicians can reduce device lead times from weeks to days.
Traditional analog workflows are linear and friction-heavy: physical impressions, stone models, shipping to labs, manual fabrication, and return shipment, often with iterative refitting. Digital workflows eliminate these bottlenecks. Anatomical data acquired via CT or intraoral scanning is transmitted directly into design pipelines and manufacturing hubs, allowing production to occur in parallel with clinical planning.
In mature digital environments, a scan obtained in the morning can be segmented, designed, and queued for manufacturing the same day, dramatically shortening the overall cycle.
These principles are now well established in cranioplasty, orthopedic surgical guides, and maxillofacial reconstruction, where patient-specific implants and guides that once took weeks can now be produced in days without delaying surgery.²,³
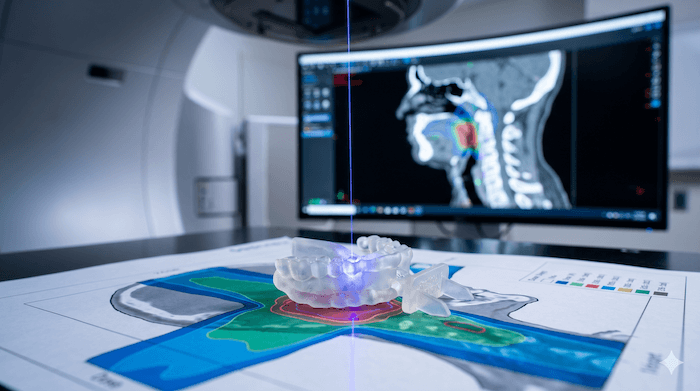
Case Example: Head & Neck Radiation and Oral Immobilization
Head and neck radiotherapy presents unique challenges due to the proximity of the tongue, mandible, and salivary glands to target volumes. Historically, clinicians relied on generic bite blocks or manually fabricated dental stents to displace oral structures—solutions that often involved:
- Lead times: 7–14 days
- Fit variability: dependent on manual fabrication
- Chairside adjustment: frequently required
Modern digital approaches have changed this equation. Using intraoral or CT-based scans and distributed manufacturing, patient-specific oral stents can now be produced in approximately 72 hours and delivered in time for simulation or early treatment fractions. Clinical benefits described in the literature include:
- Reduced dose to the tongue and oral mucosa
- Improved setup reproducibility across fractions
- Lower rates of severe oral mucositis in selected populations⁶,⁷
Importantly, these devices are present during CT simulation, fully captured in the planning dataset, and treated as passive intraoral accessories—requiring no changes to treatment planning systems or delivery parameters.
The Future of Point-of-Care Manufacturing
The prevailing model emerging in 2026 is neither fully in-house nor fully outsourced. Instead, it is a hub-and-spoke distributed manufacturing model, where:
- Clinical sites perform scanning and clinical decision-making
- FDA-registered, ISO 13485–compliant partners handle manufacturing and quality systems
This approach allows hospitals to benefit from rapid turnaround without assuming the operational and regulatory burden of running industrial manufacturing programs internally.
Regulatory guidance around additive manufacturing has matured, providing clearer pathways for patient-matched devices. Combined with established reimbursement mechanisms, this clarity has accelerated adoption beyond early adopters.
Conclusion
The story of 2025 was not about whether personalized devices could be made, it was about whether they could be delivered fast enough to matter clinically.
Digital scan-to-print workflows have closed the gap between customization and urgency. In head and neck oncology, this means clinicians no longer need to choose between starting treatment promptly and protecting patients from long-term toxicity.
As we enter 2026, the defining question is no longer “Can this be personalized?” It is “Can it be ready when the patient needs it?”
For the first time, the answer is yes.
References
- Coherent Market Insights. 3D Printing in Healthcare Market Size & Forecast, 2025–2032.
- Rosenthal G, et al. Rapid prototyping in cranioplasty. Neurosurgical Focus. 2014.
- Pfeifer R, et al. Digital vs. analog fabrication of surgical guides. 3D Printing in Medicine. 2024.
- Chen Z, et al. Waiting time for radiotherapy and outcomes. Radiotherapy and Oncology. 2008;87:3–16.
- Murphy CT, et al. Time to treatment initiation in head & neck cancer. Journal of Clinical Oncology. 2016;34:169–178.
- Yang W, et al. Custom oral stents in head and neck radiotherapy. Frontiers in Oncology. 2023.
- Verrone JR, et al. Oral stents and toxicity reduction. Radiation Oncology. 2021;16:89.